Enhance your health with free online physiotherapy exercise lessons and videos about various disease and health condition
Groin Muscle Injury
Groin Muscle Injury is also known as Adductor Strain, Groin Pull, groin strain, groin tear and pulled groin muscle. Adductor Strain is common injury in sports that involve sudden changes of direction. The onset is acute and pain is usually well localized, either to the belly of adductor longus, the proximal musculotendinous junction or the tendon near its origin on the inferior pubic ramus.
Adductor Strain (Pulled groin muscle)
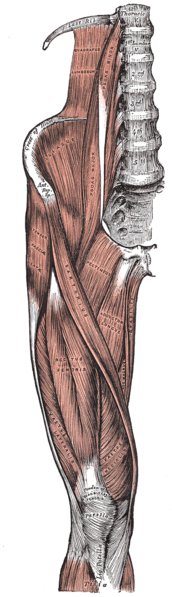
The adductor longus, adductor magnus, adductor brevis, pectineal and gracilis muscles are all adductors of the hip. Adductor strains are the most common cause of groin and hip pain in athletes, with the adductor longus the most often injured in sports.
Groin Muscle Injury or Adductor Strain Causes
Adductor strain is caused by a sudden change in direction, sprinting, forced external rotation of an abducted leg, a powerful abduction stress during simultaneous adduction while performing a cutting movement, or repetitive abduction of the free leg in a skating stride. A disparity in strength between the adductor muscles and intrinsic muscle tightness can also cause strain. Adductor strains are most commonly seen in the sports of hockey and soccer.
Groin Muscle Injury is often divided into three grades of severity:
- 1st grade: Groin Pain, but little loss of strength or movement.
- 2nd grade: Groin Pain and some tissue damage.
- 3rd grade: Groin Pain, loss of function, and a complete tear of the muscle.
Adductor Strain Differential diagnosis
Differential diagnosis of groin strain includes avascular necrosis (AVN), femoral neck stress fracture, iliopsoas/ iliopectineal bursitis, osteitis pubis, osteoarthritis, pelvic stress fracture, hernia, and athletic pubalgia.
Groin Muscle Injury or Groin Pull Symptoms
In acute injury, athletes will complain of immediate pain piercing into the groin, inability to continue the activity, swelling, and bruising. Delayed ecchymosis and soft tissue swelling may also occur.
Physical examination of groin tear will reveal tenderness to palpation along the subcutaneous border of the pubic ramus and along the involved adductor muscles and tendons, pain with resisted adduction, and pain with passive stretching.
Adductor Squeeze Test
This is done with the patient lying on the table and squeezing a ball between knees with the legs extended then done with the feet up on the table and the knees bent to 45 degrees. The third and final position is feet off bench with hips at 90 degrees. It is necessary to test all three positions, as acute tears may actually be pain-free in one of these testing positions. The purpose of these tests is to qualify pain and inhibition at all testing positions.
Adductor Strain Diagnosis
Although the diagnosis is usually made clinically, radiograph scan be helpful in excluding fractures or avulsions. If the diagnosis is still in question, magnetic resonance imaging (MRI) can be used to confirm muscle strain or partial or complete tendon tears. The most common site of strain is the musculotendinous junction of the adductor longus or gracilis.
Groin Muscle Injury or Adductor Strain Treatment
Treatment depends on the severity of the symptoms. For immediate relief of a Groin Muscle Injury, use the R.I.C.E treatment method. Rest, ice, compression, elevation are the best immediate treatment for pulls and strains and nonsteroidal anti-inflammatory drugs (NSAIDs) provide symptomatic relief.
The goal of physical therapy in adductor strain is to restore the range of motion, to prevent atrophy, and to regain strength, flexibility, and endurance. Therapy should be instituted as soon as groin pain allows and should initially include isometric contractions without resistance, followed by isometric contractions against resistance, limited by pain. Athletes can begin a stretching program after the inflammation subsides. Applying heat increases the extensibility of the collagen in the tendons and muscles and will be beneficial during this point in rehabilitation. Maintaining cardiovascular fitness with aerobic exercises that do not exacerbate the pain should be encouraged. The Physical therapy regimen in Groin Muscle Injury or Adductor Strain is summarized below.
1. 0-48 hours
- RICE
- Active pain free exercises
2. After first 48 hours Gradually increase strengthening adductor exercises
- active abduction/adduction
- adduction/flexion against resistance (rubber tubes, pulleys, light weights)
- stabilizing exercises ( pulleys with other leg, one leg squat)
3. Functional Strengthening
- bike
- pool running
- jogging
- swimming
4. Sports Specific Skills
- running- straight line
- running- figure of eight
- rapid change of direction
- kicking gradually increase
Prevention and correction of predisposing bio-mechanical factors should be included in the rehabilitation program. When the athlete has regained 70% of his or her strength and pain-free full range of motion, return to play may be allowed. This return may take 4–8 weeks for acute injuries and up to 6 months for chronic strains.
Chronic Adductor Strain or Chronic Groin Muscle Injury
Athletes with chronic adductor longus strains that have failed several months of conservative therapy have been shown to do well after surgical tenotomy and should be referred to a sports medicine orthopedic surgeon for this consideration. Complete tears of the tendinous insertion from the bone are relatively rare and generally do better with surgical repair.
Recurrent Adductor Strain
Recurrent adductor strains are common. This may be due to inadequate rehabilitation of the initial injury, resuming sports too quickly or not resolving associated problems such as lumbar spine stiffness or pelvic imbalance. If untreated, these injuries can lead to chronic exercise related groin pain.
In order to find the cause of adductor abnormalities in running athletes, it may be necessary to analyse running technique. The adductors play a major role in dampening the contraction of the gluteus medius after the propulsion phase of running. They also work synergistically with the hip abductors to maintain the stability of the pelvis during the stance phase. Thus, pelvic stability is required to prevent excessive eccentric load on the adductors.
Research Articles
- Maffey L, Emery C. What are the risk factors for groin strain injury in sport? A systematic review of the literature. Sports Med. 2007;37(10):881-94.
- Timothy F. Tyler, MS, PT, ATC, Holly J. Silvers, MPT. Groin Injuries in Sports Medicine. Sports Health. May 2010; 2(3): 231–236. [PubMed]
- Hölmich P1, Larsen K, Krogsgaard K, Gluud C. Exercise program for prevention of groin pain in football players: a cluster-randomized trial. Scand J Med Sci Sports. 2010 Dec;20(6):814-21.
Return from Groin Muscle Injury to home page
Return from Groin Muscle Injury to Sports Physical Therapy
Recent Articles
|
Author's Pick
Rating: 4.4 Votes: 252 |


 About Prodyut Das (PT, DPT) Physical Therapist at SMC, New York, USA. Former PT Winner Regional Health, South Dakota, Former HOD Physiotherapy & Fitness center @ NIMT Hospital, Greater Noida. Former PT ISIC Hospital. DPT ( Univ of Montana), MPT (neuro), MIAP, cert. manual therapist, Medical Neuroscience (USA). Licensed Physical Therapist in NY and Texas, USA. |
Connect with me- |
© Copyright physiotherapy-treatment.com since 2009 |