Enhance your health with free online physiotherapy exercise lessons and videos about various disease and health condition
Sternoclavicular Joint & Injury
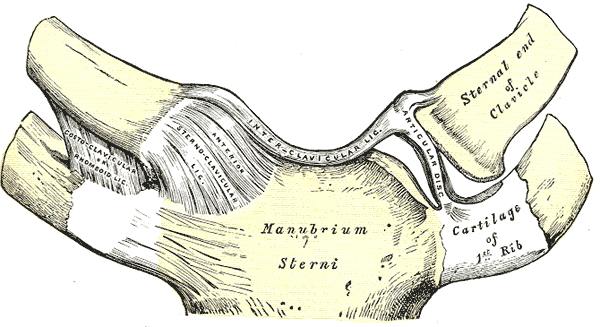
The sternoclavicular joint is a diarthrodial joint composed of the large medial end of the clavicle, the sternum, and the first rib. The joint surfaces are relatively flat and extremely incongruous, with little inherent bony stability. A fibrocartilaginous disk provides further cushioning and stability for this joint, which is surrounded by a strong series of ligaments. The anterior and posterior capsular ligaments provide the major support. The posterior portion of the capsular ligament is stronger and heavier and provides the primary support against downward displacement of the lateral clavicle. These strong ligaments attach primarily to the epiphysis of the medial clavicle, which helps to explain why medial clavicular physeal injuries in children are more common than true sternoclavicular dislocations. In addition to the capsular ligaments, the intra-articular disk ligament is a dense fibrous structure extending from the first rib through the joint and attaching through the disk to the strong capsular ligaments. Further stability for the joint is provided by the interclavicular ligament and costoclavicular ligaments. The interclavicular ligament runs from clavicle to clavicle, attaching to the superior aspect of the manubrium. The costoclavicular ligaments run from the first rib to the inferior surface of the medial clavicle. They help suspend the clavicle much like the boom of a crane.
Most clavicular motion occurs through the sternoclavicular joint. This joint has the capability of allowing 30 to 35 degrees of upward clavicular elevation (pivot), 35 degrees of anterior to posterior glide (translation), and 45 to 50 degrees of rotation about the long axis of the clavicle. This motion is extremely important for normal shoulder function as the scapula rotates to allow normal abduction and elevation of the arm. In addition to its important function in mobility, this joint provides the only true bony articulation between the upper extremity and the axial skeleton. Its position anterior to the mediastinum also gives it a protective function. In posteriorly displaced fractures and dislocations around the medial clavicle and sternoclavicular joint, injury can occur to the major neurovascular structures exiting the mediastinum.
Biomechanics of Sternoclavicular Joint
The sterno-clavicular joint is a shallow, relatively incongruous joint supported by a strong ligamentous complex. The sterno-clavicular joint is oriented somewhat posterior, lateral, and upward. It contains an intra-articular disk or meniscus that helps provide congruity and stability. Four main ligamentous groups provide support for the sternoclavicular joint. The anterior capsule is supported by anterior sternoclavicular ligaments, which provide support against anterior translation of the joint. Posteriorly, the capsule is supported by the posterior sternoclavicular ligament and the costoclavicular ligament that extends from the first rib to the clavicle. The posterior capsular ligament is the most important in supporting the shoulder against downward-oriented forces. The interclavicular ligaments extend from clavicle to clavicle across the superior manubrium and provide superior constraint. The costoclavicular ligaments run from the first rib to the inferior surface of the medial clavicle. With the arm adducted to the side, these ligaments are tightened; with the arm elevated, they are lax. Most clavicular motion occurs through the sterno-clavicular joint. Motion at the sternoclavicular joint includes about 30 to 35 degrees of upward rotation (pivot), 35 degrees of anterior to posterior glide (translation), and up to 45 to 50 degrees of axial rotation. Stability at the joint is provided by tightening of ligaments opposite the direction of motion.
Mechanism Of Injury
Because this joint is subject to practically every motion of the upper extremity and because the joint is so small and incongruous, one would think that it would be the most commonly dislocated joint in the body. However, the ligamentous supporting structure is so strong and so designed that it is one of the least commonly dislocated joints in the body. Traumatic dislocation of the sterno-clavicular joint usually occurs only after tremendous forces, either direct or indirect, have been applied to the shoulder.
- Direct Force
- Indirect Force
Most Common Cause of Injury to the Sternoclavicular Joint
The most common cause of dislocation of the sternoclavicular joint is vehicular crashes; the second is an injury sustained during participation in sports.
Classification of Injuries of the Sternoclavicular Joint
There are two types of classifications. One is based on the cause of the dislocation, and the other on the anatomic position that the dislocation assumes.
Classification Based on Anatomy
Detailed classifications are confusing and difficult to remember, and the following classification is suggested.
Anterior Dislocation
The anterior dislocation is the most common type of sternoclavicular dislocation. The medial end of the clavicle is displaced anteriorly or anterosuperiorly to the anterior margin of the sternum.
Posterior Dislocation
Posterior sternoclavicular dislocation is uncommon. The medial end of the clavicle is displaced posteriorly or posterosuperiorly with respect to the posterior margin of the sternum.
Classification Based on Cause
Traumatic Injury
Sprain or Subluxation
Acute sprains to the sternoclavicular joint can be classified as mild, moderate, or severe. In a mild sprain, all the ligaments are intact, and the joint is stable. In a moderate sprain, there is subluxation of the sterno-clavicular joint. The capsular, intra-articular disk, and costoclavicular ligaments may be partially disrupted. The subluxation may be anterior or posterior. In a severe sprain, there is complete disruption of the sternoclavicular ligaments, and the dislocation may be anterior or posterior.
Acute Dislocation
In a dislocated sternoclavicular joint, the capsular and intra-articular ligaments are ruptured. Occasionally, the costoclavicular ligament is intact but stretched out enough to allow the dislocation.
Recurrent Dislocation
If the initial acute traumatic dislocation does not heal, mild to moderate forces may produce recurrent dislocations. This is a rare entity.
Unreduced Dislocation
The original dislocation may go unrecognized, it may be irreducible, or the physician may decide not to reduce certain dislocations.
Atraumatic Problems
For a variety of nontraumatic reasons, the sternoclavicular joint may sublux or enlarge.
Spontaneous Subluxation or Dislocation
One or both of the sternoclavicular joints may spontaneously sublux or dislocate anteriorly during overhead motion. The problem is usually not painful.
Congenital or Developmental Subluxation or Dislocation
Congenital defects with loss of bone substance on either side of the joint can predispose to subluxation or dislocation.
Signs and Symptoms of Injuries of the Sternoclavicular Joint
Mild Sprain
In a mild sprain, the ligaments of the joint are intact. The patient complains of a mild to moderate amount of pain, particularly with movement of the upper extremity. The joint may be slightly swollen and tender to palpation, but instability is not noted.
Moderate Sprain (Subluxation)
A moderate sprain results in a subluxation of the sterno-clavicular joint. The ligaments are either partially disrupted or severely stretched. Swelling is noted, and pain is marked, particularly with any movement of the arm. Anterior or posterior subluxation may be obvious to the examiner when the injured joint is compared with the normal sterno-clavicular joint.
Severe Sprain (Dislocation)
A severe sprain is analogous to a joint dislocation. The dislocation may be anterior or posterior. The capsular ligament and the intra-articular disk ligament are ruptured. Regardless of whether the dislocation is anterior or posterior, there are characteristic clinical findings of sterno-clavicular joint dislocation.
Signs Common to Both Anterior and Posterior Injuries
The patient has severe pain that is increased with any movement of the arm, particularly when the shoulders are pressed together by a lateral force. The patient usually supports the injured arm across the trunk with the normal arm. The affected shoulder appears to be shortened and thrust forward when compared with the normal shoulder. The head may be tilted toward the side of the dislocated joint. The patient’s discomfort increases when he or she is placed into the supine position, at which time it will be noted that the involved shoulder will not lie back flat on the table.
Signs and Symptoms of Anterior Injury
The medial end of the clavicle is visibly prominent anterior to the sternum and can be palpated anterior to the sternum. It may be fixed anteriorly or may be quite mobile.
Signs and Symptoms of Posterior Injury
The patient with a posterior dislocation has more pain than a patient with anterior sternoclavicular dislocation. The anterosuperior fullness of the chest produced by the posteriorly dislocated clavicle is less prominent and visible compared with the normal side. The usually palpable medial end of the clavicle is displaced posteriorly. The corner of the sternum is easily palpated compared with the normal sterno-clavicular joint. Venous congestion may be present in the neck or in the upper extremity. Breathing difficulties, shortness of breath, or a choking sensation may be noted. Circulation to the ipsilateral arm may be decreased. The patient may have difficulty swallowing or a tight feeling in the throat, may be in a state of complex shock, or may have a pneumothorax.
Radiographic Evaluation of Injuries of the Sternoclavicular Joint
Anteroposterior Views
Special Projected Views
- Heinig View
- Hobbs View
- Serendipity View
Special Techniques
- Tomograms
- Magnetic Resonance Imaging
- Computed Tomography
Treatment of Traumatic Injuries
Mild Sprain
- The joint is stable but painful. Application of ice for the first 12 to 24 hours followed by heat is helpful.
- The upper extremity should be immobilized in a sling for 3 to 4 days, and then, gradually, the patient can regain use of the arm in everyday activities.
Moderate Sprain (Subluxation)
- For subluxation of the sterno-clavicular joint, application of ice is recommended for the first 12 hours, followed by heat for the next 24 to 48 hours.
- The joint may be subluxed anteriorly or posteriorly, and the subluxation may be reduced by drawing the shoulders backward as if reducing and holding a fracture of the clavicle.
- A clavicle strap can be used to hold the reduction. A sling and swath should also be used to hold up the shoulder and to prevent motion of the arm. The patient should be protected from further possible injury for 4 to 6 weeks.
- Repair of the ligaments and temporary internal fixation of the sternoclavicular joint with pins drilled from the clavicle into the sternum may be done. Postoperatively, a plaster figure-of-eight cast can be appied and, in addition, support it with a sling and swathe. The pins and the cast are removed after 6 weeks.
Severe Sprain (Dislocation)
The dislocation of the sternoclavicular joint may be anterior or posterior.
Nonoperative Treatment
- Anterior Dislocation-Technique of Closed Reduction
- Posterior Dislocation-Techniques of Closed Reduction
Technique of Operative Treatment
- Surgical Reconstructions
- fascia lata between the clavicle and the sternum.
- subclavius tendon be used to reconstruct a new costoclavicular ligament
- Osteotomy of the Medial Clavicle
- Resection of the Medial End of the Clavicle
- Arthrodesis
Treatment of Atraumatic Problems
Read research articles about Sternoclavicular joint on PubMed
Congenital or Developmental Conditions
Congenital or developmental problems (e.g., absencenor partial absence of bone or muscles) can produce subluxation or dislocation of the sterno-clavicular joint. Specific rehabilitation or surgical procedures are not usually necessary.
Arthritis
The management of patients with osteoarthritis can usually be done with conservative nonoperative treatment; that is, heat, anti-inflammatory agents, and rest. However, the patient must be thoroughly evaluated to rule out other conditions that mimic the changes in the sterno-clavicular joint (e.g., tumor, metabolic, infectious, or collagen disorders). Patients with post-traumatic arthritic changes in the sterno-clavicular joint, which follow fractures of the sternoclavicular joint and previous attempts at reconstruction, may require a formal arthroplasty of the joint and careful stabilization of the remaining clavicle to the first rib.
Return from sternoclavicular joint to Home Page
Return from sternoclavicular joint to Physiotherapy links
Recent Articles
|
Author's Pick
Rating: 4.4 Votes: 252 |


 About Prodyut Das (PT, DPT) Physical Therapist at SMC, New York, USA. Former PT Winner Regional Health, South Dakota, Former HOD Physiotherapy & Fitness center @ NIMT Hospital, Greater Noida. Former PT ISIC Hospital. DPT ( Univ of Montana), MPT (neuro), MIAP, cert. manual therapist, Medical Neuroscience (USA). Licensed Physical Therapist in NY and Texas, USA. |
Connect with me- |
© Copyright physiotherapy-treatment.com since 2009 |