Enhance your health with free online physiotherapy exercise lessons and videos about various disease and health condition
Anterior Cord Syndrome
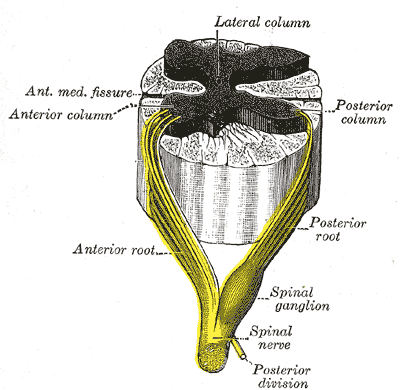
The anterior cord syndrome (also known as Beck's syndrome or anterior spinal artery syndrome) involves a lesion affecting the anterior two-thirds of the spinal cord while preserving the posterior columns. It may occur with retropulsed disc or bone fragments, direct injury to the anterior spinal cord, or with lesions of the anterior spinal artery which provides the blood supply to the anterior spinal cord. There is a variable loss of motor as well as pinprick sensation with a relative preservation of light touch, proprioception, and deep-pressure sensation. Patients usually have a 10% to 20% chance of muscle recovery.
Cause
Traumatic. This syndrome may result from a forced flexion, compression injury which may occur in diving or road traffic accidents (Foo et al 1981).
Non-traumatic. The anterior cord syndrome may result from infarction secondary to anterior spinal artery thrombosis, spinal cord angioma or rupture of aortic aneurysm. Significant neurological recovery following spinal cord infarct is unusual unless there is improvement within the first 24 hours (Geldermacher & Nager 1989; cited in Stevenson et al 1996).
Clinical Picture of Anterior Cord Syndrome
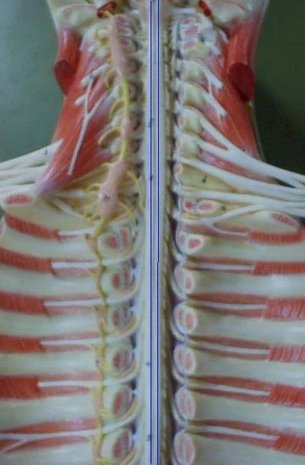
This syndrome results from damage to the anterior part of the spinal cord.
The clinical signs and symptoms are those of:
The severity of impairment will depend upon the extent and exact site of the damage. Patients presenting with motor loss and sensory sparing are classified as Frankel B, or B on the ASIA impairment scale. However, these scales make no distinction between the types of sensory sparing, e.g. tactile, joint position sense and pain and temperature.
A clear distinction has been made between the different types of sensory sparing. Those with preserved pin prick have been shown to have an excellent prognosis to regain a functional gait. Crozier et al (1991) found that 66% of Frankel B patients with preservation of pin perception recovered to become functional walkers, whereas only 14% with light touch were able to walk (n = 33).
Vibration sense, tactile and joint position sense are served by the dorsal columns, whereas pain and temperature sensation is dependent upon the spinothalamic tracts. Preservation of pin prick indicates some integrity of the spinothalamic tracts in the anterolateral aspect of the spinal cord and therefore the possibility of some sparing of the adjacent corticospinal tracts (Foo et al1981).
Body awareness enables patients with anterior cord lesions to respond more quickly to the rehabilitation process, often achieving their treatment goals in a shorter time. However, management of these patients is the same as that for Frankel A patients. Continuous pain has been identified as a key feature following spinal cord infarction (PeIser & van Gijn 1993).
Sensory sparing clearly indicates that the lesion is incomplete, but a significant difference in outcome to those with incomplete lesions is only possible where there is some motor recovery.
SCI Related Pages







Further Reading
- Anterior spinal artery syndrome. From Wikipedia, the free encyclopedia
- Anterior-Cord-Syndrome. Apparelyzed.com
- Dr Yuranga Weerakkody and Dr Prashant Mudgal et al. Anterior-cord-syndrome. Radiopaedia.org
- Spinal Cord Injury. American Association of Neurological Surgeons
- William McKinley, MD, Katia Santos, MD, Michelle Meade, PhD, and Karen Brooke, MT. Incidence and Outcomes of Spinal Cord Injury Clinical Syndromes. J Spinal Cord Med. 2007; 30(3): 215–224.
Return From Anterior Cord Syndrome to Home Page
Return From Anterior Cord Syndrome to Neuro Rehab

 About Prodyut Das (PT, DPT) Physical Therapist at SMC, New York, USA. Former PT Winner Regional Health, South Dakota, Former HOD Physiotherapy & Fitness center @ NIMT Hospital, Greater Noida. Former PT ISIC Hospital. DPT ( Univ of Montana), MPT (neuro), MIAP, cert. manual therapist, Medical Neuroscience (USA). Licensed Physical Therapist in NY and Texas, USA. |
Connect with me- |
© Copyright physiotherapy-treatment.com since 2009 |